RTs are responsible for holding c-spine when moving or rolling a trauma patient whose spine has not been cleared
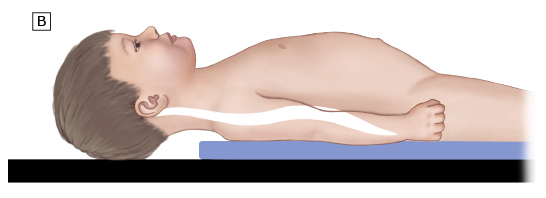
When immobilizing the c-spine, first the patient must be in a neutral cervical spine position. For babies and small children this is what is known as the “sniffing position”, they will need padding/board under their shoulders, torso and legs.
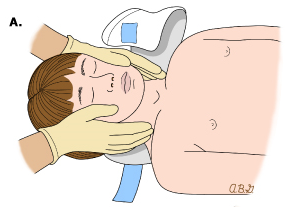
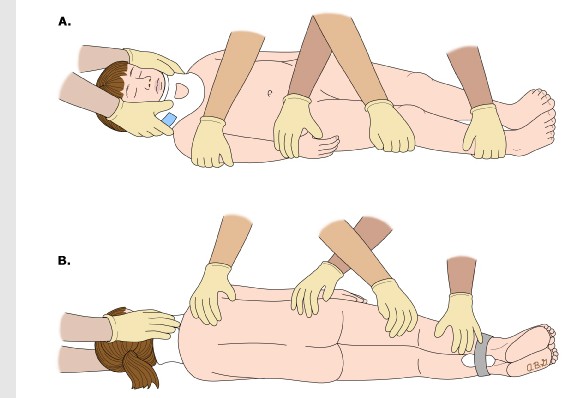
One person should solely be responsible for maintaining the cervical spine in neutral position for repositioning the patient. Log rolling procedure should be used when moving patient with c-spine precautions.
The c-collar should be a snug fit, staff should be able to fit 2 fingers under collar and be able to feel carotid pulse.
Pediatric Glasgow Coma Scale (GCS)
Used to describe the general level of consciousness in pediatric patients with traumatic brain injury (TBI) and to define broad categories of head injury
The GCS is divided into 3 categories
Eye opening (E)
Eyes opening spontaneously
Eye opening to speech
Eye opening to pain
No eye opening or response
Motor response (M)
Smiles, oriented to sounds, follows objects, interacts
Cries but consolable, inappropriate interactions
Inconsistently inconsolable, moaning
Inconsolable, agitated
No verbal response
Verbal response (V)
Infant moves spontaneously or purposefully
Infant withdraws from touch
Infant withdraws from pain
Abnormal flexion to pain for an infant (decorticate response)
Extension to pain (decerebrate response)
No motor response
The score is determined by the sum of the score in each of the 3 categories, with a maximum score of 15 and a minimum score of 3
Criteria for CAT 1 vs CAT 2 vs CAT 3 Trauma
CAT 1
Amputation proximal to the wrist or ankle
High-voltage electrical contact (greater than or equal to 220 volts)
Intracranial hemorrhage with midline shift
Penetrating wound
Head/neck
Chest/abdomen/groin
Mid-femur to shoulder
Mid-femur to groin
Open and depressed skull fracture
Arrest from blunt or penetrating trauma
Airway or ventilatory compromise
Facial/tracheal trauma
Potential inhalation injury
Intubated
Assisted ventilations
Chest wall instability or deformity
Flail chest
Any patient receiving blood products to maintain hemodynamic stability
Physiological criteria of a GCS less than 9 or deteriorating mental status
Spinal cord paralysis
Presence of a tourniquet to control bleeding
Systolic blood pressure
Less than 60 for under 1 year old
Less than 70 for 1-5 years old
Less than 80 for 6-12 years old
Less than 90 for greater than 12 years old
CAT 2
Hemothorax/Pneumothorax
Crush injuries proximal to wrist or ankle
Fall of greater than 10 feet or 3 times the child’s height
Hanging
MVC, ATV, Motorcycle, Golf cart
Ejected/separated from vehicle
Death of passenger in the same compartment
Auto vs Ped/Bicyclist thrown, run over, or with significant (greater than 20 MPH) impact
Penetrating wound to distal extremities excluding hands and feet
GCS 9-13
2nd or 3rd degree burns with greater than 20% Body surface area covered
Two or more proximal long bone fractures
CAT 3
MVC with speeds greater than 60 MPH
Snake bites with signs of envenomation
Degloving proximal to wrist or ankle
Suspected pelvic fracture
Simultaneous upper and lower extremity fractures
Suspicion for Non-Accidental Trauma
Liver/Spleen/Pancreas/renal injury without hemodynamic effects
Intracranial hemorrhage without midline shift
Roles for the 2 RTS Involved in a Trauma
RT 1
Applies lead apron under Personal Protective Equipment (PPE)
Prepares airway and intubation equipment prior to the patient’s arrival, as able
Assists the physician managing the airway with administration of oxygen or provision of assisted respiratory support if patient’s respirations are absent or inadequate
Maintains manual immobilization of the cervical spine during intubation and all procedures, or delegates this to another trauma team member as needed
Secures and reassesses tube placement throughout resuscitation and stabilization
Places ETCO2 adaptor and connect to the monitor for an intubated patient
Monitors ETCO2 and pulse oximetry and patient’s response to interventions
Initiates mechanical ventilation during evaluation and stabilization of the patient, if indicated
Assists with the transfer of intubated patient to radiology, CT scan, OR, PICU or Special Procedures
From position at the patient’s head, offers comfort and reassurances to the injured child and explains procedures as patient’s condition allows
RT 2
Assists ED Respiratory Therapist & Airway Physician with management of airway
Locates and prepares non-invasive airway options or ventilator as needed
Communicates with Trauma Team Leader to verify ETT placement after X-ray obtained
Runs blood gases as ordered, reports results to Trauma Team Leader