The right atrium receives oxygen-poor blood from the superior and inferior vena cava and pumps it to the right ventricle through the tricuspid valve. The right ventricle pumps the oxygen-poor blood through the pulmonary valve into the pulmonary arteries and then into the lungs. The left atrium receives oxygen-rich blood from the pulmonary veins and pumps it to the left ventricle through the mitral valve. The left ventricle pumps the oxygen-rich blood through the aortic valve and out to the rest of the body through the aorta
Superior and inferior vena cava to right atrium to tricuspid valve to right ventricle to pulmonary valve to pulmonary arteries to lungs to pulmonary veins to left atrium to mitral valve to left ventricle to aortic valve to aorta to body
Overall goal of the cardiorespiratory system
to provide the organs and tissues of the body with an adequate supply of oxygen in relation to oxygen consumption (VO2)
SVO2
The amount of oxygen remaining in the systemic venous blood after blood passes through the organs and tissues throughout the body
Reflects the balance between oxygen supply and demand
Normal is 20 points lower than Spo2, which is normally 60-80%
If there is a LOW SVO2 WITH NORMAL SPO2 then the cardiac output is not high enough to meet tissue oxygen needs, so the tissues are extracting a higher percentage of oxygen from the blood than normal
Two components that make up oxygen delivery
Cardiac output
Arterial oxygen content
Ventilator desynchronycan lead to Increases oxygen consumption
If arterial oxygen content is diminished, some ways to maintain adequate oxygen deliver are
Cardiac output augmentation with preload optimization
Inotropic agents
Vasodilators
Optimization of mechanical ventilation
Mechanical cardiac support devices, when indicated
Preload
Also known as the left ventricular end-diastolic pressure (LVEDP)
The amount of ventricular stretch at the end of diastole
The heart loading up for the next big squeeze of the ventricles during systole
Afterload
Also known as the systemic vascular resistance (SVR)
The amount of resistance the heart must overcome to open the aortic valve and push the blood volume out into the systemic circulation
Stroke Volume
The amount of blood pumped by the left ventricle of the heart in one contraction. Not all the blood contained in the left ventricle, about two-thirds is expelled with each beat
Together with the heart rate, the stroke volume determines cardiac output
Diastolic Blood Pressure
Perfuses the coronary artery
If it’s too low then there’s not enough pressure to push blood flow through
Lactate
A molecule produced If oxygen isn’t available to body cells and anaerobic metabolism kicks in to produce energy
An increase in lactate production is typically caused by impaired tissue oxygenation, either from decreased oxygen delivery or a disorder in oxygen use
Most causes of lactic acidosis are due to significant, systemic tissue hypoperfusion from cardiac output not being high enough to meet tissue oxygen needs
QP:QS ratio
Pulmonary to Systemic Flow ratio
Will tell you if there is overcirculation
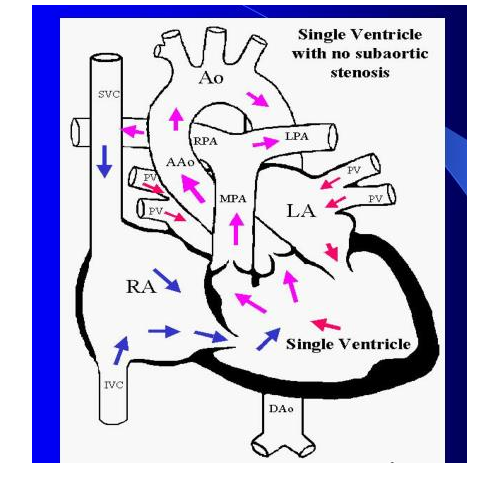
Target for single ventricle heart patients is 1:1
MIXING Cardiac Lesions
What are they
When there is left to right or right to left communication of blood flow
Examples:
Pre-op Pulmonary Atresia
Pre-op Pulmonary Stenosis
Pre-op Tricuspid Atresia
Pre-op and some Post-op Tetralogy of Fallot
Pre-op Interruption of the Aortic Arch
Pre-op Coarctation of the Aorta
Pre-op Transposition of the Great Vessels
Pre-op and Post-Op Single Ventricle
Pre-op and Post-Op Hypoplastic Left or Right hearts
How PH, CO2, and O2 affect MIXING lesions
pH
Acidosis increases Pulmonary Vascular Resistance leading to Right to Left shunting, vice versa with alkalosis
PCO2
High CO2 increases Pulmonary Vascular Resistance leading to Right to Left shunting, vice versa with decreased CO2
O2
Decreased O2 increases Pulmonary Vascular Resistance leading to Right to Left shunting, vice versa with increased O2, which can lead to Pulmonary edema
Ways to decrease PVR
Optimizing lung volume
Increasing pH
Decreasing PaCO2
Increasing PaO2
Minimizing intrathoracic pressures
BLOOD FLOW RESPONSE TO PVR when there is LEFT TO RIGHT CARDIAC COMMUNICATION
Increased PVR there will be less left to right communication
Decreased PVR leads to greater left to right communication that causes over-circulation and potential pulmonary edema
Effects of Mechanical Ventilation on the Pulmonary Vasculature
PPV can reduce right ventricular afterload in patients with low lung volume by expanding collapsed lung units and reducing PVR.
PPV can increase right ventricular afterload in conditions of pulmonary overdistention with excessive alveolar expansion and subsequent compression of the perialveolar capillaries.
Increasing the FIO2 improves PaO2 in patients without a right-to-left shunt and reduces pulmonary artery vascular resistance. Increasing inspired oxygen in patients with intracardiac shunts produces little change in PaO2; however, a reduction in PVR still results. Thus, an increase in alveolar and/or arterial oxygen content can reduce PVR.
In conditions of increased afterload, a reduction in PVR will decrease right ventricular afterload and lead to an improvement of right ventricular function. These beneficial cardiorespiratory interactions may be employed, especially after congenital heart surgery and in those with pulmonary hypertension, to assist patients with right ventricular dysfunction. Beyond the use of oxygen, inhaled nitric oxide and other pulmonary vasodilators may be employed.
PVR is not always beneficial, as can be seen in patients with large intracardiac or extracardiac shunts. The addition of inspired oxygen can reduce PVR and increase pulmonary blood flow. In conditions of decreased pulmonary flow, this may improve oxygen delivery by increasing arterial oxygen content. However, in clinical situations of increased pulmonary flow (eg, ventricular septal defect, large patent ductus arteriosus, and hypoplastic left heart syndrome), the associated increase in pulmonary blood flow can result in pulmonary over-circulation and pulmonary edema.For those patients with single-ventricle physiology, the resultant pulmonary overcirculation may occur at the expense of systemic output with a reduction in global oxygen delivery.
Effects of Ventilator Manipulations
On the Right Ventricle
Increases in intrathoracic pressure decrease cardiac output causing:
Decreases RV preload
Increases PVR
On the Left Ventricle
Increase in intrathoracic pressure increases cardiac output leading to:
Increasing LV preload when low
Increasing LV afterload
Decreasing preload when excessive (RV) effects
Cardiac Drugs
Prostin
Maintains the patency of the ductus arteriosus until corrective or palliative surgery can be performed in neonates who have congenital heart defects and who depend upon the patent ductus for survival
Milrinone
Vasodilator that relaxes the muscles in your blood vessels to help them dilate, which lowers blood pressure and allows blood to flow more easily through your veins and arteries. Used as a short-term treatment for life-threatening heart failure
Epinephrine
In the heart, it increases the rate and force of contraction, thus increasing the output of blood and raising blood pressure
Norepinephrine
Used to treat low blood pressure. works on alpha receptors only found in the arteries. can make your blood vessels become narrower, increasing blood pressure
JET (Junctional Ectopic Tachycardia)
Rare syndrome of patients recovering from heart surgery. They have a "short-circuit" in their heart, where the electricity bypasses the AV node, causing the heart to beat faster than normal
There may be an accelerated narrow complex tachycardia, usually within the first 24–48 hours after surgery
There may be atrio-ventricular disassociation with more ventricular signals than atrial signals
The cause of JET is felt to be due to manipulation of the tissue surrounding the AV node during surgery
Cardiac Anomalies
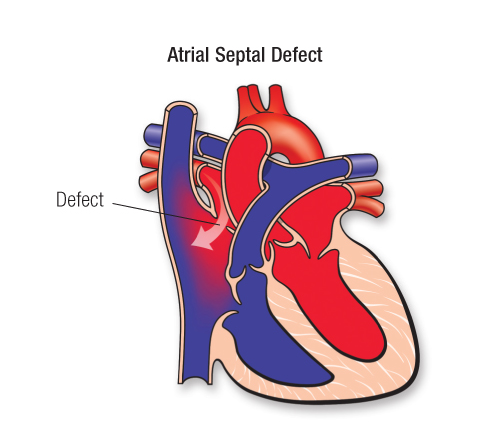
Atrial Septal Defect(ASD)
Etiology:
An opening in the atrial septum allowing direct communication between the right and left atrium.
Pathophysiology:
Results in right ventricular volume overload and increased pulmonary blood flow under low pressure. The size of the shunt is more dependent on RV compliance than the size of the defect.
If left unrepaired, ASD's can produce RA and RV dilatation and hypertrophy, atrial arrhythmias, CHF and possible paradoxical emboli.
Signs & Symptoms:
Most children are asymptomatic.
A crescendo-decrescendo type murmur is heard over the second to third intercostal space along the sternal border.
Fixed splitting of the second heart sound
With severe defects (ex. partial AV canal), signs of CHF may be noted.
CXR shows right atrial and ventricular hypertrophy.
ECG shows right atrial and ventricular enlargement.
Management:
If the infant is symptomatic, anti-congestive medications may be used to treat the symptoms of CHF and early surgical repair is recommended.
If the child is asymptomatic, closure of medium to large ASD's is recommended before school age.
Post-operative Complications:
Arrhythmias
Residual shunt
Dyspnea and exercise intolerance
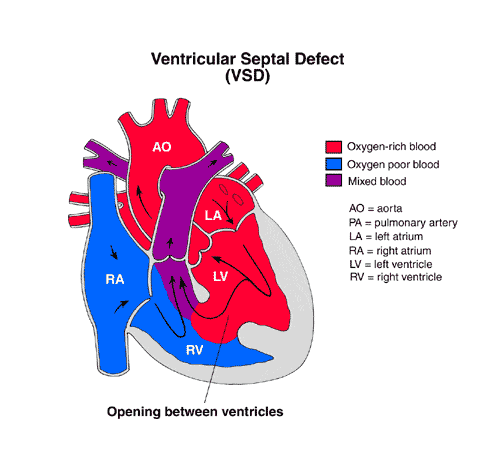
Ventricular Septal Defect (VSD)
Etiology:
The presence of an opening in the interventricular septum that allows for direct communication between the right and left ventricles.
Pathophysiology:
The amount of blood flow across a VSD is related to it's size and pulmonary vascular resistance.
Restrictive VSD - small & medium VSD's there is a pressure gradient between the ventricles with left being greater than the right. The shunt is based on the pressure gradient and the blood is delivered to the pulmonary circulation under low pressure.
Non-restrictive VSD - large VSD the ventricular pressures are equal. The shunt is based on PVR and SVR. The shunted blood is delivered to the pulmonary circulation under high pressure and can cause pulmonary hypertension.
Signs & Symptoms:
With the decrease in PVR, the shunt may increase and lead to congestive heart failure. CHF symptoms are a result of the large volume of blood being circulated to the pulmonary system and the overload of the left side of the heart. Net result is decreased peripheral perfusion and increased energy expenditure and work of breathing due to the volume overload in the pulmonary system and left heart.
QP/QS ratio describes the ratio of the pulmonary blood flow and systemic blood flow.
Small VSD's have flow ratios of 1.5 to 1
Medium VSD have flow ratios of 1.5-2 to 1
Large VSD's have flow ratios of >2 to 1
Physical exam:
Loud, harsh, pansystolic murmur heard at the left lower sternal border
Cardiomegaly by CXR
ECG shows RV hypertrophy
Management:
Indications for surgery are:
CHF that is not controlled by anti-congestive medications
Failure to thrive
Frequent respiratory infectionsInfundibular defects that show signs of aortic insufficiency
Post-operative Complications:
Congestive heart failure
Arrhythmias
Ventricular dysfunction
Low cardiac output
Pulmonary hypertension
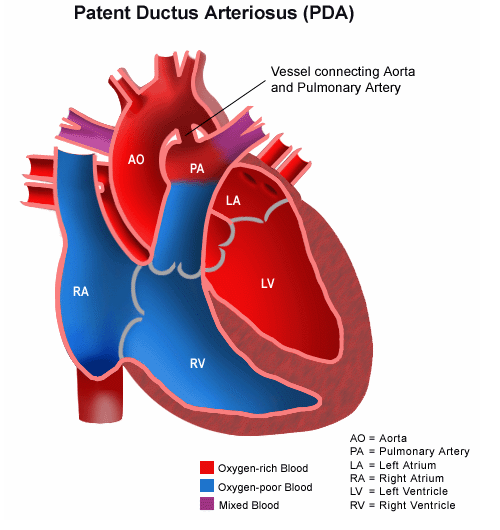
Patent Ductus Arteriosus (PDA)
Etiology:
Persistence of the fetal structure beyond the perinatal period
Normally, the ductus closes within hours of birth.
Pathophysiology:
Until PVR decreases there may be little blood shunting through the ductus.
If the PVR is greater than SVR, there may be a right to left shunt through the ductus.
As the PVR decreases, the size of the shunt will increase, potentially leading to CHF due to pulmonary over circulation.
Increased pulmonary blood flow also leads to increased work on the left side of the heart, possibly leading to LV dilation and hypertrophy.
Pulmonary over circulation can also lead to pulmonary vascular disease over time.
A PDA may also be a life-saving structure providing the only source of pulmonary blood flow with some defects.
Signs & Symptoms:
Continuous murmur heard at the second left intercostal space along themid clavicular line.
Signs of CHF
Bounding peripheral pulses and a widened pulse pressure
Evidence of LV hypertrophy on CXR and ECG
Management:
Indocin (indomethacin) to cause pharmacologic closure
primarily used in premature neonates
Coil embolization
Surgical ligation and/or division
Post-operative Complications:
Complications of a thoracotomy - bleeding, atelectasis, hemothorax pneumothorax.
Phrenic or recurrent laryngeal nerve injury
Vocal cord paralysis
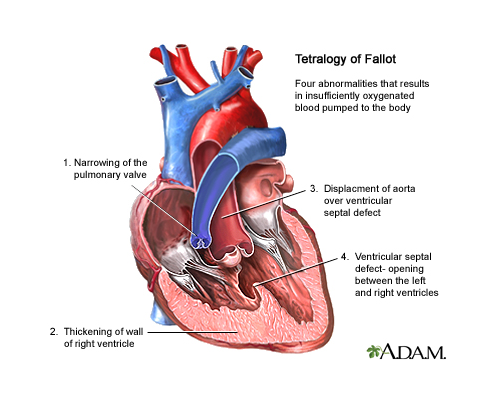
Tetralogy of Fallot (TOF)
Etiology:
The association of four cardiac abnormalities:
VSD
Pulmonary stenosis
Overriding aorta
Right ventricular hypertrophy
Pathophysiology:
The resulting hemodynamics depends on the degree of obstruction to pulmonary blood flow.
If the stenosis is mild, this may balance the shunting through the VSD and the child may be a "pink TET".
Approximately 1/4 of the children have hypercyanotic spells resulting from increased oxygen demands with limited pulmonary blood flow.
If the stenosis is severe, PVR may exceed SVR and a right to left shunt (RV to aorta) may occur.
Signs & Symptoms:
The degree of cyanosis observed is related to the severity of the pulmonary stenosis.
Newborns usually show minimal cyanosis because the PDA is providing another source of pulmonary blood flow.
On exam - a systolic ejection murmur heard at the second intercostal space along the left sternal border.
The goal of repair is to close the VSD and reconstruct the pulmonary outflow tract, possibly with a transannular patch.
Post-operative Complications:
Congestive heart failure from RV dysfunction
Residual obstruction to pulmonary blood flow
LV dysfunction, or a residual VSD
Low cardiac output
Bleeding
Arrhythmias (increased incidence with transannular patch)
Neurological complications
Single Ventricle
Etiology:
A group of congenital defects characterized by the presence of a single ventricle that receives both systemic and pulmonary venous blood.
The associated atrioventricular inlets and morphology usually categorize these defects.
The most common is the double inlet left ventricle.
Pathophysiology:
If there is obstruction to pulmonary blood flow, severe cyanosis will be present from birth. Pulmonary blood flow may be dependent on a PDA.
If there is no obstruction to pulmonary blood flow, severe hypoxemia may not be observed.
As PVR decreases, signs of CHF may be observed.
Signs & Symptoms:
Clinical signs depend on three factors:
Volume of pulmonary blood flow
The mixing of systemic and pulmonary venous blood
The presence of significant associated lesions.
Management:
With obstruction to pulmonary blood flow:
PGE to maintain ductal patency
A shunt to secure pulmonary blood flow is often needed in the new born period
Without obstruction to pulmonary blood flow:
Treat symptoms of CHF as the PVR decreases
Usually these children are repaired surgically with a Fontan or modified Fontan
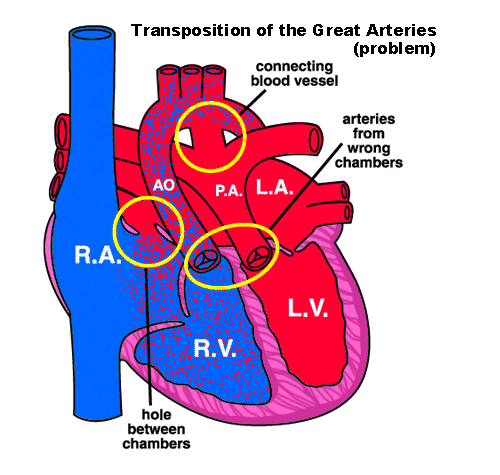
Transposition of the Great Arteries (TGA)
Etiology:
Results from inappropriate septation and migration of the truncus arteriosus during fetal development.
The aorta arises off the right ventricle and the pulmonary artery arises off the left ventricle.
Unless there is some means for mixing of blood, there are two separate circulations and this defect is fatal.
Sites for mixing are a PDA, ASD and VSD.
Pathophysiology:
The degree of arterial oxygen desaturation depends on the amount of mixing of systemic and pulmonary venous blood and the amount of effective pulmonary blood flow.
Usually the ductus stays patent for several days after birth due to the desaturation. As the pulmonary vascular resistance decreases, signs of CHF may be observed in infants with large VSD's.
Signs & Symptoms:
Cyanosis and acidosis with the closure of the PDA
Signs of CHF with the decrease of PVR if there is a large VSD
A murmur is not heard in about half of these children or a systolic murmur may be heard
CXR may show a normal sized heart if there is no VSD
ECG shows right ventricular hypertrophy and possibly biventricular hypertrophy with a VSD
Management:
PGE drip and initial stabilization.
A Rashkind septostomy may be done to increase mixing at the atrial level.
Surgical repairs:
Arterial Switch (Jantene) procedure - returns the great vessels to their normal anatomic relationship with the ventricles.
Venous Switch - redirects the flow of venous return within the atria.
Post-operative Complications:
Arterial Switch - low cardiac output
Bleeding
Arrhythmias
Neurological complications
Kinking or stenosis of the coronary arteries leading to myocardial ischemia